
We now have the most authoritative estimate of the value provided by wearing masks during the pandemic: approximately zero. The most rigorous and extensive review of the scientific literature concludes that neither surgical masks nor N95 masks have been shown to make a difference in reducing the spread of Covid-19 and other respiratory illnesses.
This verdict ought to be the death knell for mask mandates, but that would require the Centers for Disease Control (CDC) and the rest of the public-health establishment to forsake “the science”—and unfortunately, these leaders and their acolytes in the media seem as determined as ever to ignore actual science. Before the pandemic, clinical trials repeatedly showed little or no benefit from wearing masks in preventing the spread of respiratory illnesses like flu and colds. That was why, in their pre-2020 plans for dealing with a viral pandemic, the World Health Organization, the CDC, and other national public-health agencies did not recommend masking the public. But once Covid-19 arrived, magical thinking prevailed. Officials ignored the previous findings and plans, instead touting crude and easily debunked studies purporting to show that masks worked.
The gold standard for medical evidence is the randomized clinical trial, and the gold standard for analyzing this evidence is Cochrane (formerly the Cochrane Collaboration), the world’s largest and most respected organization for evaluating health interventions. Funded by the National Institutes of Health and other nations’ health agencies, it’s an international network of reviewers, based in London, that has partnerships with the WHO and Wikipedia. Medical journals have hailed it for being “the best single resource for methodologic research” and for being “recognized worldwide as the highest standard in evidence-based healthcare.”
It has published a new Cochrane review of the literature on masks, including trials during the Covid-19 pandemic in hospitals and in community settings. The 15 trials compared outcomes of wearing of surgical masks versus wearing no masks, and also versus N95 masks. The review, conducted by a dozen researchers from six countries, concludes that wearing any kind of face covering “probably makes little or no difference” in reducing the spread of respiratory illness.
It may seem intuitive that masks must do something. But even if they do trap droplets from coughs or sneezes (the reason that surgeons wear masks), they still allow tiny viruses to spread by aerosol even when worn correctly—and it’s unrealistic to expect most people to do so. While a mask may keep out some pathogens, its inner surface can also trap concentrations of pathogens that are then breathed back into the lungs. Whatever theoretical benefits there might be, in clinical trials the benefits have turned out to be either illusory or offset by negative factors. Oxford’s Tom Jefferson, the lead author of the Cochrane review, summed up the real science on masks: “There is just no evidence that they make any difference. Full stop.”
This lack of evidence would be enough to keep any new drug or medical treatment from being approved—much less one whose purported benefits had not even been weighed against the harmful side effects. As the Cochrane reviewers disapprovingly note, few of the clinical trials of masks even bothered to collect data on the harmful effects on subjects. Most public-health officials and journalists have ignored the downsides, too, and social-media platforms have censored evidence of those harms. But there’s no doubt, from dozens of peer-reviewed studies, that masks cause social, psychological, and medical problems, including a constellation of maladies called “mask-induced exhaustion syndrome.”
Yet public-health officials, in violation of the first-do-no-harm principle, continue recommending or mandating masks without good evidence of their effectiveness or any pretense of cost-benefit analysis. Masks are still required in many hospitals and other institutions. Despite all the data showing that Covid-19 poses virtually no risk to healthy children, the CDC continues to recommend masking all students in communities where infection rates are rising. While the WHO advises against masks for children under six, and the European Union advises against them for students under 12, the CDC cruelly recommends masking everyone from age two on up.
The CDC’s director, Rochelle Walensky, remains determined to ignore the best research on masks, as she made clear in a congressional hearing earlier this month. “Our masking guidance doesn’t really change with time,” she said when asked how the new review from Cochrane would affect the agency’s policies. “This is an important study,” she conceded, “but the Cochrane review only includes randomized clinical trials, and, as you can imagine, many of the randomized clinical trials were for other respiratory viruses.”
It was a statement remarkable for its chutzpah as well as its scientific incoherence. One of the worst mistakes of the CDC and other lavishly funded federal agencies was the failure to conduct randomized clinical trials to determine whether their policies were effective. The Cochrane review had to rely on pandemic mask trials conducted in other countries—and now Walensky has the gall to complain that other countries didn’t do enough of the research that U.S. agencies shirked. She’s right that some of the trials involved other viruses, but why dismiss them as irrelevant to the coronavirus? And while one can always wish for more studies to include in a meta-analysis, that’s no excuse to ignore the best available evidence in favor of the shoddy science peddled by her agency to defend its policies.
Early in the pandemic, the CDC justified its newfound enthusiasm for masks in a press release hailing “the latest science” from a case study of a hair salon in Missouri. “Wearing a mask prevented the spread of infection from two hair stylists to their customers,” the CDC proclaimed, a preposterously sweeping conclusion to draw from a small observational study that lacked a control group and had other obvious limitations (most of the salon’s customers were never even tested for Covid). On national television, Walensky touted another study, of schools in Arizona, as proof that masks dramatically reduced the spread of Covid, but the study’s methodology was so clearly flawed—and the results so out of line with rigorous studies—that other Covid researchers dismissed it as “ridiculous” and “so unreliable that it probably should not have been entered into the public discourse.”
Instead of sponsoring—or at least heeding—clinical trials, the CDC kept searching for confirmation from less reliable research. It repeatedly cherry-picked observational data, crediting masks for a short-term reduction in Covid rates in some localities while ignoring contrary data from more systematic analyses, such as a study that tracked rates nationwide over the entire first year of the pandemic—and found that neither mask mandates nor mask usage correlated with infection rates.
Can anything persuade the maskaholics in the public-health establishment and the public to give up their obsession? Some researchers, echoing Walensky, concede that the Cochrane review is the gold standard but argue that the clinical trials so far haven’t been extensive enough to rule out the possibility that masks might do some good. But that vague possibility is no reason to force masks on people: a public-health intervention is supposed to be based on solid evidence, not wishful thinking.
In his book Unmasked: The Global Failure of COVID Mask Mandates, data analyst Ian Miller devotes an entire chapter to graphs exposing the CDC’s statistical malfeasance. He also prepared a graph for a previous City Journal article that is worth showing again, because it’s a visual confirmation—from nationwide data, not clinical trials—of the conclusions in the Cochrane review. The graph tracks the results of the natural experiment that occurred across the United States in the first two years of the pandemic, when mask mandates were imposed and lifted at various times in 39 states.
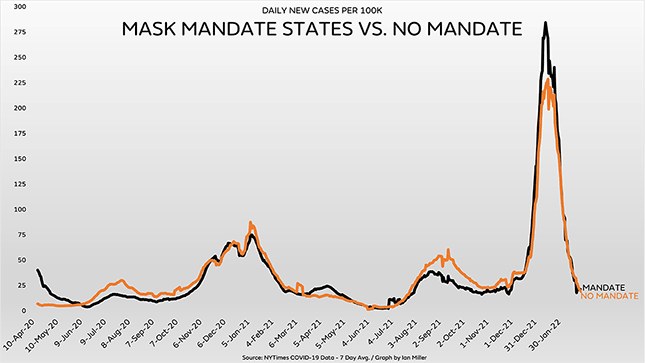
The black line on the graph shows the weekly rate of Covid cases in states with mask mandates that week, while the orange line shows the rate in states without mandates. As you can see, the trajectories are virtually identical, and if you add up all those numbers, the cumulative rates of Covid cases are virtually identical, too. So are the cumulative rates of Covid mortality (the mortality rate is actually a little lower in the states without mask mandates). Hundreds of millions of Americans dutifully covered their faces in the states with mandates, and the result was the same as in the clinical trials analyzed by Cochrane: the masks made no difference.
Photo by FREDERIC J. BROWN/AFP via Getty Images